


Advancing Health Obsequity
Suppression, Subservience, and Stifling of Inquiry

In the 1950s, songwriter/comedian Tom Lehrer, describing a fictional character, said, “Like so many contemporary philosophers, he especially enjoyed giving helpful advice to people who were happier than he was.” In the 2020s, those who seek to “moderate” public discourse especially enjoy giving helpful advice to people who are more articulate, coherent, and open-minded than they are. An iconic example, though not unique, is Advancing Health Equity: A Guide to Language, Narrative and Concepts (AHE)—a 54-page catalogue of linguistic do’s and don’ts for medical students and practicing physicians. Issued in 2021 by the Association of American Medical Colleges and the American Medical Association, the document is a recipe for stifling scientific discourse and doctor-patient conversations—a labyrinth of conversational speed bumps, potholes, detours, checkpoints, and barricades.
It would take far more than 54 pages to describe all that is wrong with this particular speech code. I mentioned AHE recently in my Substack journal (“Medical Heretics from Rome to COVID”) and wrote at length about it in 2021 (“The Pall of Politics Descends Upon American Medicine”). In both cases, I cited one specific recommendation that illustrates both the risible and ruinous aspects of the guide. Below, we’ll explore that example in some depth.
Before proceeding, let’s clarify a few things. Racism and other bigotries exist. Sometimes they’re subconscious. Bigotries can and do impact people’s health. So can incentives baked into atavistic institutional structures. Doctors can be boorish and insensitive. However, it does not follow logically that hectoring, incomprehensible, ideology-soaked speech diktats will mitigate these problems. In the 20th Century, such diktats forced medicine into destructive adamance on topics as diverse as genetics, autism, ulcers, and neurodegenerative disorders. Eugenic orthodoxies permeated medical training, resulting in unprecedented violations of human rights. More recently, lives were damaged and lost because legitimate lines of inquiry on COVID were declared taboo.
The Closing of the Scientific Mind
AHE’s Table 5 is titled “Contrasting Conventional (Well-intentioned) Phrasing with Equity-focused Language that Acknowledges Root Causes of Inequities.” Borrowed from a National Association of County and City Health Officials (NACCHO) document, it offers the following sentence as “Conventional” phrasing:
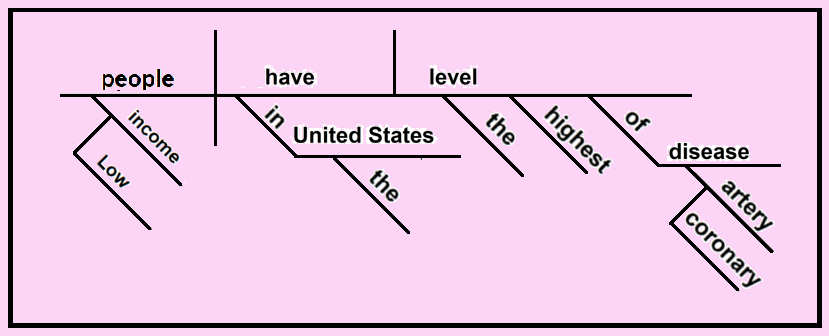
“Low-income people have the highest level of coronary artery disease in the United States.”
In place of this straightforward, 15-word, 27-syllable sentence, AHE (via NACCHO) recommends the following 39-word, 78-syllable pilgrimage, which it labels “Equity-focused Language that Acknowledges Root Causes of Inequities”:
“People underpaid and forced into poverty as a result of banking policies, real estate developers gentrifying neighborhoods, and corporations weakening the
power of labor movements, among others, have the highest level of coronary artery disease in the United States.”
Reed-Kellogg sentence diagrams are a useful, albeit somewhat out-of-fashion, tool for visualizing the structure of writing. To read what follows here, you don’t need any background in this technique. The diagrams simply offer a pictorial representation of how Advancing Health Equity brings meaningful conversation to a halt.
Here’s the original sentence—a neat, compact elocution. The leftmost third tells us that we’re talking about “low-income people.” In the middle, we see that such people “in the United States have” something. The rightmost segment says that this something which they possess is “the highest level of coronary artery disease” in the country. This is a concise, coherent, comprehensible declaration expressing an observable empirical regularity.
This formulation leaves the clinician or researcher wide latitude to inquire into the nature of this statistical relationship. In treating a low-income patient with coronary artery disease, for example, a clinician can ask a great number of questions in order to craft a patient-specific treatment regimen:
Why is a particular patient’s income low? Did she throw away a Harvard physics scholarship so she could live on a commune and make candles? Could her capacity to work have been limited by a debilitating rock-climbing injury? Does she have a congenital neurological condition that impairs her ability to work? Was her reputation destroyed on the internet by a misogynistic boyfriend? Did racism derail her early intellectual promise? Is she a recent immigrant who only recently restarted her life in America? Was she financially ruined by gambling or bad investments? Or is she just kind of lazy?
What is the relationship between this patient’s income status and cardiac condition? Is it more accurate to say that: (A) her coronary artery disease resulted from her low-income status? (B) her low-income status resulted from the coronary artery disease? (C) her low-income status and coronary artery disease sprang from some common cause? or (D) her low-income status and coronary artery disease are coincidental?
What factors other than income might have contributed to this patient’s cardiac status? Was she born into a family that has a genetic predisposition for such illness? Has she been noncompliant with prescribed medical regimens? If so, might this noncompliance be related to her low-income status? Does she smoke, use drugs, or drink to excess? Has she tended toward unhealthy eating habits? Did she fail to exercise regularly?
A doctor who sees each patient as an individual can consider all of these and fine-tune medical advice to match the fine-grained specifics of the patient at hand. A researcher investigating a whole population can explore the interaction of all these different causal factors. This is the stuff of science.
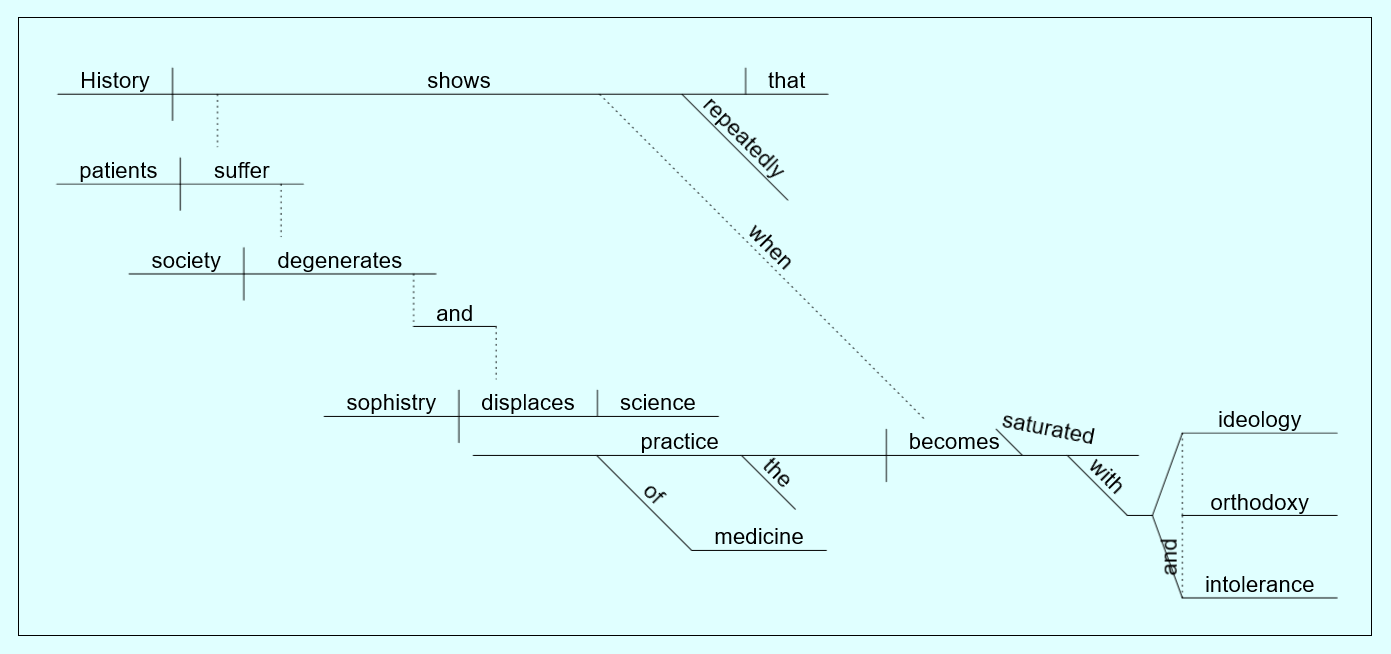
In contrast, consider AHE’s suggested “revision”:

The sentence represented by Figure 2’s “equity-focused language” closes the door on most scientific questions. It starts with the spare facts of Figure 1 and then takes the reader on an extended stream-of-consciousness side journey—effectively shutting down many questions that clinicians and researchers might want to ask. Let’s look at how that happens.

VICTIMHOOD: The red box (#1) in Figure 3 strips away the patient’s personal agency. By fiat, she is absolved of any responsibility for her income level and declared a victim—purposefully impoverished by nefarious forces. Someone underpaid her and forced her into poverty. In its persistently purple prose, AHE suggests that this hapless innocent is a victim of “structural violence.” AHE also decries “the overwhelming focus on changing individual behavior to improve health, mostly avoiding the social and economic conditions which generate poor health outcomes—this individualistic focus reflects dominant narratives.” The effective message is: if you’re poor and sick, it’s not your fault, and it’s not your responsibility to make things better. Of course, sometimes that’s true, but AHE makes it the general, if not universal case.
VILLAINY: The blue box (#2) identifies the villains who have heaped poverty and illness on the patient. While the field of economics has vast literatures on the factors that determine incomes and poverty, AHE has narrowed it down to three primal causes—bankers, real estate developers, and corporations, whose machinations provide the One True Explanation of sickness. This monomaniacal explanation is as unscientific as the long-held belief that all illness derives from an imbalance of bodily humors.
VIOLATIONS: The green boxes (#3) further zero in on the specifics of causality—gentrification and union-busting. These, along with banking policies, are the violations by which they impoverish and sicken innocent, blameless people. The scientific literatures of economics and medicine are jettisoned in favor of an ideology-drenched single-bullet theory.
VERTIGO: The brown box (#4) informs us what has happened (“coronary artery disease”) to the subjects (“people”) whom this sentence last mentioned 27 words and a maze of accusatory assertions ago. This is comically awful writing—the maundering that one expects in software manuals and remedial writing classes.
Speech codes are only one aspect of an ongoing process of infantilizing medical students—reducing would-be healers to toddlers in scrubs. So are ideological litmus tests for med school applicants, mandatory catechisms to fashionable ideologies, authoritarian content moderation on social media platforms, and obsequious fealty to professors’ viewpoints. Science, as opposed to scientism, cannot flourish in such an atmosphere. As a linguistic exercise, I leave it to readers—particularly those associated with medical schools and institutions—to decipher the sentence represented by Figure 4.
Robert F. Graboyes publishes Bastiat’s Window, a Substack journal of economics, science, and culture—with an emphasis on healthcare. He is a health economist, journalist, and musician in Alexandria, Virginia, and holds five degrees, including a PhD in economics from Columbia University. In 2014, he received the Reason Foundation’s Bastiat Prize for Journalism. His music compositions are at YouTube.com/@RFGraboyes/videos.

As I read ‘Bastiat’ this morning I thought to myself this Graboyes fellow--as learned and clever as I’ve come to appreciate he is--has gone too far to make his point. No one in their right mind will believe his spoof of the medical establishment....
but then I realized, holy🤬
(all my thoughts that followed have been redacted to protect your reader’s sensibilities)
This should be required reading for all med school faculty and officers of the AMA and the AAMC